Trade Screen Time for Sunshine: Why Kids Should Stay Active This Summer
Summer break is finally here! For many kids, that means sleeping in, relaxing, and having plenty of free time. While it’s tempting to spend hours playing video games, watching videos, or scrolling on tablets, summer is the perfect opportunity to get outside and stay active.
The Benefits of Being Active
Physical activity helps kids stay healthy, strong, and energized. Running, biking, swimming, playing sports, or even walking around the neighborhood can improve fitness, build muscle strength, and support healthy growth. Active kids often sleep better and have more energy throughout the day.
Being active also benefits mental health. Outdoor play can reduce stress, improve mood, and boost self-confidence. Fresh air and sunshine help children feel happier and more focused compared to spending long periods indoors staring at screens.
Why Too Much Screen Time Can Be a Problem
Technology can be fun and educational, but too much screen time can have negative effects. Spending hours on devices may lead to less physical activity, poor posture, eye strain, and difficulty sleeping. Excessive screen use can also take away valuable opportunities for social interaction and creative play.
When kids spend most of their summer in front of a screen, they may miss out on memorable experiences that help build important life skills such as teamwork, problem-solving, and communication.
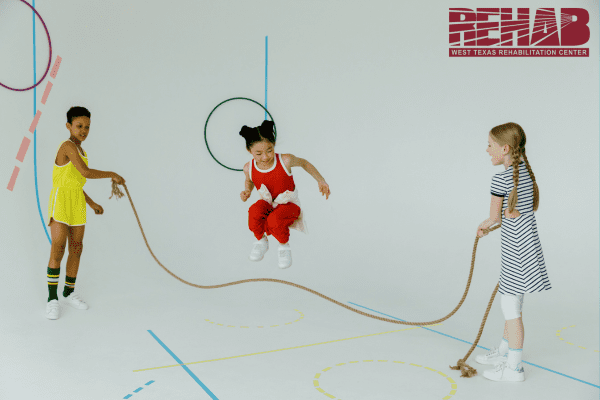
Fun Ways to Stay Active This Summer
The good news is that staying active doesn’t have to feel like exercise. Here are some fun ideas:
- Ride a bike around the neighborhood.
- Visit a local park or playground.
- Play soccer, basketball, or another favorite sport.
- Go swimming with family or friends.
- Create a backyard obstacle course.
- Take nature walks and explore local trails.
- Play tag, hide-and-seek, or other outdoor games.
- Help with gardening or yard work.
Even simple activities can make a big difference when done regularly.
Finding a Healthy Balance
Summer should be about enjoying a variety of activities. Screens don’t have to disappear completely, but setting limits can help create a healthy balance. Try scheduling outdoor play before screen time or setting daily goals for physical activity.
Parents can encourage active habits by joining in the fun. Family walks, bike rides, and outdoor games create lasting memories while helping everyone stay healthy.
Make This Summer Count
Summer only comes once a year, and it’s a great time for kids to explore, play, and stay active. By spending less time on screens and more time moving, kids can enjoy better health, stronger friendships, and unforgettable adventures. So put down the device, head outside, and make this summer your most active one yet!